Are We Starting Horses Too Young? What the Science Actually Says
Few topics ignite more debate in the horse world than the question of when a young horse should begin work. On one side, there’s concern that starting too early risks long-term soundness issues. On the other, some argue that thoughtful early training may actually support bone development. So instead of arguing from a point of instinct or tradition, I think it’s time to take a look at what the research actually says.
𝐆𝐫𝐨𝐰𝐭𝐡 𝐏𝐥𝐚𝐭𝐞 𝐂𝐥𝐨𝐬𝐮𝐫𝐞 𝐢𝐧 𝐇𝐨𝐫𝐬𝐞𝐬
Let’s begin by addressing the color-coded diagram of an equine skeleton that frequently circulates social media. This diagram illustrates when growth plates close, which begins in the lowest parts of each limb and moves up the skeleton sequentially, ending at the spine. This diagram is popular as many use it to justify recommendations on when to start horses.
I decided to do some digging to track down the origin of this information, and my investigation led me to a table in a book that was published in 1975. This table cites literature that evaluated the closure of the epiphyseal growth plate in the appendicular skeleton (forelimbs and hindlimbs) through radiographs (Getty, 1975).
Since then, a review by Rogers et al. (2021) was published and concluded that the majority of growth for horses is completed by the time they are 2 years old. Additional research evaluating the vertebrae suggest that longitudinal growth of the spine ceases when wither height growth is complete (Butler et al., 1993). Based on these findings, the reviewers suggested that starting horses at the age of 2 is an acceptable practice that aligns with their developmental potential.
But that begs the question whether we should base recommendations on growth plate activity and active bone growth or on growth plate fusion and closure – as these are two very different metrics. This was detailed in a presentation by Collar et al. (2020) in which growth plate activity of lumbosacral vertebrae in Quarter Horses stopped when horses were 2 years old but growth plate closure or fusion was not complete until horses were between 2 and 8 years old.
𝐒𝐨 𝐰𝐡𝐢𝐜𝐡 𝐦𝐞𝐚𝐬𝐮𝐫𝐞𝐦𝐞𝐧𝐭𝐬 𝐬𝐡𝐨𝐮𝐥𝐝 𝐰𝐞 𝐮𝐬𝐞 𝐚𝐧𝐝 𝐰𝐡𝐚𝐭 𝐝𝐨𝐞𝐬 𝐭𝐡𝐞 𝐫𝐞𝐬𝐞𝐚𝐫𝐜𝐡 𝐬𝐚𝐲?
When evaluating race horses, Santschi et al. (2017) found that horses who began training at 2 years of age did not have a higher risk of injury during their racing careers. In fact, they tended to have more successful careers including more lifetime starts, wins, earnings, and years raced.
At first glance, it may seem counterintuitive. But young, growing bodies are built to adapt and specifically, bone development is supported by high cellular activity, an active periosteum, abundant blood supply, and open growth plates. As the body matures, it gradually shifts from a state of building to maintaining. Hormonal changes occur, bones become less adaptable, and osteoblasts (bone-building cells) struggle to keep pace with osteoclasts (cells that break bone down).
In other words – the window for skeletal adaptation is early and we accept this reality in humans all the time.
Young athletes routinely begin training long before their growth plates close. Elite gymnasts, swimmers, and figure skaters often compete internationally as teenagers. Many children enter organized sports as early as five or six years old despite the fact that human growth plates typically remain open until they are 14 to 17.
𝐒𝐨 𝐰𝐡𝐲 𝐝𝐨𝐞𝐬 𝐞𝐚𝐫𝐥𝐲 𝐰𝐨𝐫𝐤 𝐢𝐧 𝐡𝐨𝐫𝐬𝐞𝐬 𝐩𝐫𝐨𝐯𝐨𝐤𝐞 𝐬𝐮𝐜𝐡 𝐬𝐭𝐫𝐨𝐧𝐠 𝐫𝐞𝐬𝐢𝐬𝐭𝐚𝐧𝐜𝐞 𝐰𝐡𝐞𝐧 𝐢𝐭 𝐢𝐬 𝐚𝐜𝐜𝐞𝐩𝐭𝐚𝐛𝐥𝐞 𝐟𝐨𝐫 𝐡𝐮𝐦𝐚𝐧𝐬?
I believe the controversy is not tied to the work itself, but rather the conditions surrounding the work.
Youth athletes are typically offered diversity in the exercise they are allowed to complete, do not have to carry an external load, and can refuse participation or voice concerns. Youth sports are also framed as a crucial part of both physical development and confidence building.
In comparison, young horses are often subjected to repetitive, discipline-specific movement, asked to carry a rider, tend to be confined outside of training, and have no autonomy regarding their participation. Equine sports, specifically those centered around young horses, tend to be tied to economic benefits, tradition, and human timelines that do not always put the horse first.
I believe this is where we have significant room for improvement in the equine industry.
Another consideration is the amount of research we have to provide recommendations. There are a wide variety of breeds and disciplines in the equine industry and the current data is not representative of all demographics. Additionally, for many, performance outcomes aren’t the whole picture. And at the moment, equine research does not extend past a horse’s athletic career, so we may not currently grasp long-term implications of early work.
𝐁𝐮𝐭 𝐭𝐡𝐢𝐬 𝐢𝐬 𝐰𝐡𝐞𝐫𝐞 𝐰𝐞 𝐜𝐚𝐧 𝐮𝐬𝐞 𝐡𝐮𝐦𝐚𝐧 𝐫𝐞𝐬𝐞𝐚𝐫𝐜𝐡 𝐭𝐨 𝐨𝐟𝐟𝐞𝐫 𝐮𝐬 𝐚 𝐮𝐬𝐞𝐟𝐮𝐥 𝐩𝐞𝐫𝐬𝐩𝐞𝐜𝐭𝐢𝐯𝐞.
One of the clearest risks in youth athletics isn’t early movement, it’s repetition without variation.
While sports offer health benefits, single-sport specialization in children has been strongly linked to higher injury rates (Jayanthi et al., 2019). These risks are associated with children performing the same movements repetitively, which puts stress on the same joints and strains the same muscles.
Overuse injuries are especially likely during rapid growth phases, when muscle imbalances and coordination shifts are common (Arnold et al., 2017). This is because active growth is often tied to bone growth that outpaces muscles and tendon development. This imbalance can result in tight muscles, reduced flexibility, and structural instability, which temporarily declines coordination and balance and increases the risk of injury.
Youth athletes also face an increased risk of early-onset osteoarthritis which is linked to high-impact activities, repetitive movements, and severe joint injuries, all of which can accelerate cartilage degeneration (Saxon et al., 1999). However, osteoarthritis wasn’t identified until later in life due to a higher pain tolerance in youth and the time it takes for the condition to develop. I believe a long-term study evaluating this relationship in horses would be extremely insightful.
𝐒𝐨 𝐭𝐡𝐞 𝐢𝐬𝐬𝐮𝐞 𝐢𝐬𝐧’𝐭 𝐬𝐢𝐦𝐩𝐥𝐲 𝐰𝐡𝐞𝐭𝐡𝐞𝐫 𝐲𝐨𝐮𝐧𝐠 𝐛𝐨𝐝𝐢𝐞𝐬 𝐬𝐡𝐨𝐮𝐥𝐝 𝐰𝐨𝐫𝐤 𝐛𝐮𝐭 𝐡𝐨𝐰 𝐭𝐡𝐞𝐲 𝐰𝐨𝐫𝐤.
The key takeaway is that early training is not inherently harmful, rather the structure and approach to that training are what make the difference.
Variety is critical. Cross-training helps distribute stress across tissues and reduces the risk created by repetitive movement patterns. Youth athletes who were highly specialized in a single sport were almost twice as likely to sustain an overuse injury compared to someone competing in multiple sports (Bell et al., 2018). Trail rides, cavaletti work, or practicing a new discipline are all opportunities to not only improve musculoskeletal health but also support a horse’s mental wellbeing.
Short, intentional bouts of higher-intensity loading may stimulate bone adaptation more effectively than long periods of low-intensity exercise – as bone requires a dynamic strain above threshold to elicit bone formation. This was demonstrated by a study evaluating endurance horses completing ‘long, slow’ work, which found that horses in endurance training did not increase bone strength compared to horses allowed to freely exercise on pasture (Spooner et al., 2008).
Meanwhile, sprint exercises have been shown to result in greater bone strength (Logan et al., 2019), increased endosteal circumference (Firth et al., 2012), and greater bone mineral content (Hiney et al., 2004). However, balance is critical. When young horses were sprinted excessively, it had harmful impacts on joint health as the horse was responding to an unnatural amount of work (Van de Lest et al., 2002). While we still need to determine the appropriate level of high-impact work for horses, one study found that just one sprint a week could increase bone strength (Logan et al., 2019).
Load matters, too, and some weight-bearing can be beneficial. Research found that horses carrying 100 lbs while trotting had greater bone mineral deposition of the cannon bone compared to those who did not carry weight (Nielsen et al., 2002). However, it is important to note that the load these horses carried does not reflect most riding situations. In comparison, excessive loads could be detrimental to the horse and rider size is a real consideration when starting young horses.
Movement also builds coordination, balance, and proprioception. Expecting a horse to enter athletic work at maturity without foundational motor skills would be like asking a 22-year-old to learn and compete in a sport like soccer or gymnastics against someone who has trained since childhood. Early exposure to low-intensity technical challenges such as balance, body awareness, and varied terrain, can be incredibly valuable.
𝐀𝐧𝐝 𝐩𝐞𝐫𝐡𝐚𝐩𝐬 𝐦𝐨𝐬𝐭 𝐢𝐦𝐩𝐨𝐫𝐭𝐚𝐧𝐭𝐥𝐲: 𝐥𝐢𝐟𝐞𝐬𝐭𝐲𝐥𝐞 𝐦𝐚𝐭𝐭𝐞𝐫𝐬.
Work is only a small part of a horse’s day.
A two-year-old that is lightly trained but lives in turnout and is allowed to move freely, navigate space, and engage in natural behaviors, is experiencing something very different from one that lives in a stall for the majority of the day.
This is backed by research in which young horses pastured for at least 12 hours a day had greater bone mineralization and cannon bone circumference in comparison to their counterparts who lived in a stall (Bell et al., 2001). Since young horses often live in stalls during sale prep or once they enter training, they may be more likely to have bone loss or an increased risk of injuries. While that stall may be convenient for us, movement outside of structured exercise is critical for musculoskeletal development as well as mental wellbeing.
𝐀𝐫𝐞 𝐰𝐞 𝐚𝐬𝐤𝐢𝐧𝐠 𝐭𝐡𝐞 𝐫𝐢𝐠𝐡𝐭 𝐪𝐮𝐞𝐬𝐭𝐢𝐨𝐧?
Perhaps the real issue isn’t if young horses should work or even what age to start them, but whether the work we ask of them is age-appropriate.
Most horses are still in an active growth phase until around 2 years of age, and during this time, structured work should be limited while free movement through pasture turnout may be the most appropriate and beneficial form of loading.
Once rapid growth begins to slow, workload can be introduced thoughtfully and tailored to the individual, taking into account breed, maturity, and current developmental stage. At this point, how we develop the horse matters far more than simply when we begin.
𝐂𝐨𝐧𝐜𝐥𝐮𝐬𝐢𝐨𝐧
If I had to summarize some recommendations, they would include:
House your horse in a pasture or paddock over a stall.
Cross train to reduce the risk of overuse injuries.
Focus on low intensity, technical work at a young age to improve coordination and proprioception.
Utilize high-intensity work strategically to increase bone strength.
Minimize work during any growth spurts.
Make decisions for your specific horse based on individual growth and characteristics.
The bottom line is that early work itself isn’t the issue – what really matters is how young horses are trained, managed, and allowed to live.
If you want to read more on this topic, I encourage you to read an open access review (which means it is accessible to everyone!) by Logan and Nielsen (2021) which highlighted a lot of the research I covered in this post. I will include a link in the comments!
There’s always more to unpack, but hopefully this reframes the conversation in a way that allows us to use science to mold our decisions instead of tradition.
Cheers,
Dr. DeBoer
Reining Trainers Enigma’s Conclusion:
Starting 2yo is not the problem. The problems are:
References:
Table 15-2; Getty R(ed): Sisson and Grossman’s The Anatomy of the Domestic Animals , ed 5. Philadelphia , WB Saunders Co , 1975, p 272.
Rogers CW, Gee EK, Dittmer KE. Growth and bone development in the horse: when is a horse skeletally mature?. Animals. 2021 Nov 29;11(12):3402.
Butler, J.A., Colles, C.M., Dyson, S., Kold, S., Poulos, P. Clinical Radiology of the Horse. 1993.
Collar, E. M., Russell, D. S., Huber, M. J., Duesterdieck-Zellmer, K. F., & Stover, S. M. (2020). Investigation into lumbosacral vertebral anatomy and growth plate closure in Quarter Horses [Video]. AAEP Proceedings. American Association of Equine Practitioners.
Santschi, E.M.; White, B.J.; Peterson, E.S.; Gotchey, M.H.; Morgan, J.M.; Leibsle, S.R. Forelimb Conformation, Sales Results, and Lifetime Racing Performance of 2-Year-Old Thoroughbred Racing Prospects Sold at Auction. J. Equine Vet. Sci. 2017, 53, 74–80.
Jayanthi NA, Post EG, Laury TC, Fabricant PD. Health consequences of youth sport specialization. Journal of athletic training. 2019 Oct 1;54(10):1040-9.
Arnold A, Thigpen CA, Beattie PF, Kissenberth MJ, Shanley E. Overuse physeal injuries in youth athletes: risk factors, prevention, and treatment strategies. Sports health. 2017 Mar;9(2):139-47.
Saxon L, Finch C, Bass S. Sports participation, sports injuries and osteoarthritis: implications for prevention. Sports medicine. 1999 Aug;28(2):123-35.
Bell DR, Post EG, Biese K, Bay C, Valovich McLeod T. Sport specialization and risk of overuse injuries: a systematic review with meta-analysis. Pediatrics. 2018 Sep 1;142(3):e20180657.
Spooner HS, Nielsen BD, Woodward AD, Rosenstein DS, Harris PA. Endurance training has little impact on mineral content of the third metacarpus in two-year-old Arabian horses. Journal of Equine Veterinary Science. 2008 Jun 1;28(6):359-62.
Logan, A., Nielsen, B., Robison, C., Manfredi, J., Schott, H.; Buskirk, D., Hiney, K. Calves, as a model for juvenile horses, need only one sprint per week to experience increased bone strength. J. Anim. Sci. 2019, 97, 3300–3312.
Firth, E.C., Rogers, C.W., Rene van Weeren, P., Barneveld, A., Wayne McIlwraith, C., Kawcak, C.E., Goodship, A.E., Smith, R.K.W. The Effect of Previous Conditioning Exercise on Diaphyseal and Metaphyseal Bone to Imposition and Withdrawal of Training in Young Thoroughbred Horses. Vet. J. 2012, 192, 34–40.
Hiney, K.M., Nielsen, B.D., Rosenstein, D. Short-Duration Exercise and Confinement Alters Bone Mineral Content and Shape in Weanling Horses. J. Anim. Sci. 2004, 82, 2313–2320.
Van de Lest, C., Brama, P.A.J., René Van Weeren, P. The Influence of Exercise on the Composition of Developing Equine Joints. Biorheology 2002, 39, 183–191.
Bell RA, Nielsen BD, Waite K, Rosenstein D, Orth M. Daily access to pasture turnout prevents loss of mineral in the third metacarpus of Arabian weanlings. Journal of animal science. 2001 May 1;79(5):1142-50.
Nielsen BD, O’Connor CI, Rosenstein DS, Schott HC, Clayton HM. Influence of trotting and supplemental weight on metacarpal bone development. Equine Veterinary Journal. 2002 Sep;34(S34):236-40.
















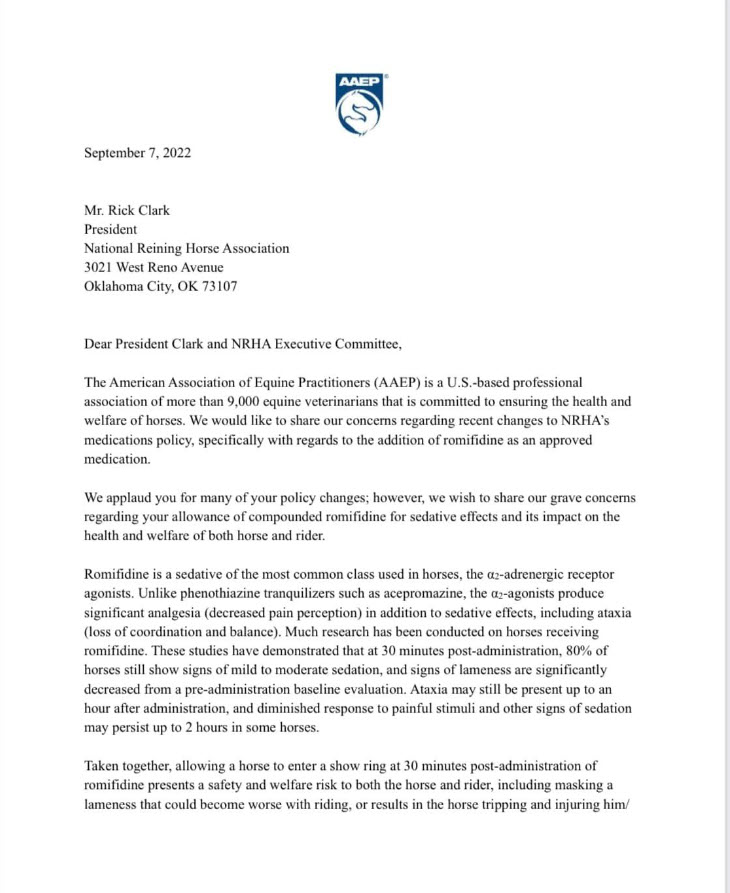
 While the NRHA is boasting about their great new penalties, are they just distracting members and the public from the fact that there is no accountability for whether violations are acted upon? History says, most unlikely. Some members say it’s just more of the same ‘mushroom syndrome’. [The practice of being supplied with little or no information and often instead intentionally supplied with misinformation]
While the NRHA is boasting about their great new penalties, are they just distracting members and the public from the fact that there is no accountability for whether violations are acted upon? History says, most unlikely. Some members say it’s just more of the same ‘mushroom syndrome’. [The practice of being supplied with little or no information and often instead intentionally supplied with misinformation]